 By: Dr. Shaina Cahill, Ph.D. (Director Of Operations and Medical Affairs)
By: Dr. Shaina Cahill, Ph.D. (Director Of Operations and Medical Affairs)
The gut microbiome has become a focus in the health and wellness space over the last two decades. With the growing awareness about the importance of gut health, the ability to augment and restore the gut microbiome has become a focus of both popular culture and science 1–6. Two ways to alter the gut microbiome that has grown in interest are probiotics and fecal microbiota transplantation (FMT), and while these two approaches might seem similar on the surface, they are actually quite different 7–14!
Probiotics and their fundamental flaw, engraftment
Probiotics are defined as living microorganisms that are intended to provide health benefits when consumed 12,13. While nothing new, probiotics have gained traction as an option to alter gut microbiota and restore balance in the gut in the 20th century 8–10,12,13. Probiotics have demonstrated an ability to restore the balance of the gut microbiota and reduce gut inflammation and associated GI symptoms, such as bowel function 8,12,13,15.
When discussing probiotics, it is important to note that probiotics do not engraft in the gut microbiome, and their effects are transient 11,16–18. This means that the bacteria in the probiotic cannot establish into the microbial community, and their effects are short-lived 11,16,18. It is also possible that probiotics can have negative effects during gut dysbiosis, as a recent study found that probiotics can actually delay the recovery of the microbiome after disruption (such as antibiotics) 16,19.
How is FMT different?
FMT, involves transferring a sample of a donor’s healthy gut microbiome, from their stool, into the gut of a recipient, with the aim of restoring a healthy gut microbial community 3,20–22. FMT has been widely and effectively used to treat recurrent Clostridium difficile infection and has shown promise in treating other conditions, such as inflammatory bowel disease 23–25, metabolic disorders 26–31, Parkinson’s disease 32–34 and autism spectrum disorder 35–37 and many more 7,20,22,29,38,39.
The main advantage of FMT over probiotics is that FMT provides a full spectrum of the microbes in the gut, and these microbes present in the donor’s sample are able to engraft and provide long-lasting changes in the gut microbiome 11,16,19,40–44. So, what does this mean?
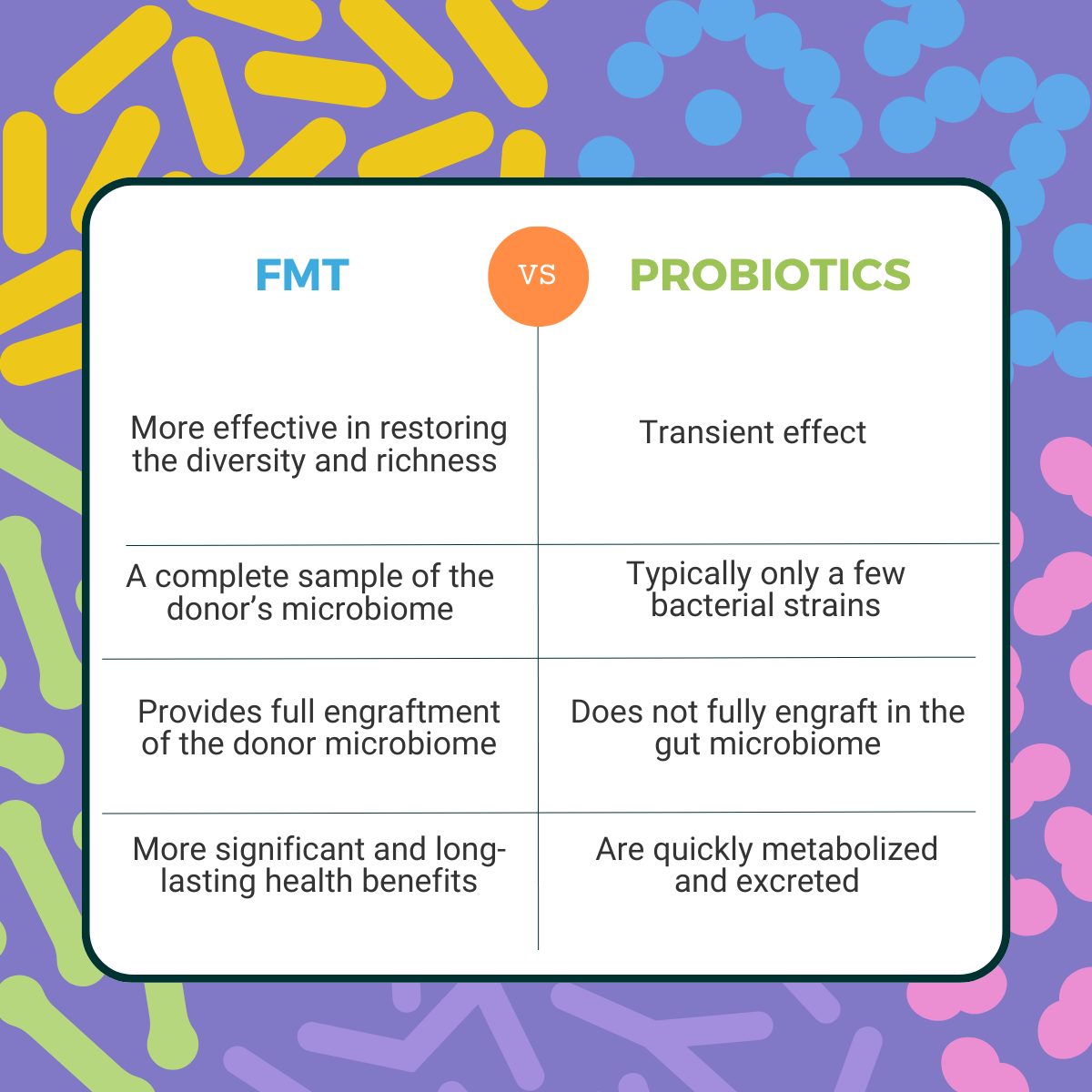
1. FMT provides a complete sample of the donor’s microbiome, whereas probiotics typically only introduce a few bacterial strains, providing a more complete and diverse microbiome than probiotics, which can lead to more significant and long-lasting health benefits 11,36,40,43–46.
2. FMT provides full engraftment of the donor microbiome, which is then populated in the recipient’s gut. FMT has been shown to be more effective than probiotics in restoring the diversity and richness of the gut microbiome 11,16,19,35,41,44,47,48.
Conclusion
While probiotics and FMT may seem similar at first glance, they are quite different in their potential benefits and effects on the gut microbiota community. While probiotics can be helpful and have benefits 8,12,13,15, their effects are transient, and they do not engraft in the gut microbiome 11,16–18. FMT, on the other hand, provides a full spectrum of the microbes in the gut and appears to be a more effective treatment for restoring gut microbiome dysfunction 11,16,36,40,43–46.
At Novel Biome, we're passionate about the importance of the gut microbiome and the transformative potential of Fecal Microbiota Transplantation (FMT) treatment to restore health. As an FMT contract manufacturer, we leverage our years of experience in FMT to manufacture high-quality FMT products utilizing our highly-screened donors and stringent manufacturing standards. If you are interested in learning more about our FMT products and manufacturing capabilities, please contact us HERE or to register as a clinical partner to order FMT products, click HERE.
Reference: 1. Bresalier, R. S. & Chapkin, R. S. 2020, 2. Hajela, N. et al. 2015, 3. Ser, H.-L. et al. 2021, 4. Thaiss, C. A. et al. 2016, 5. Thursby, E. & Juge, N. 2017, 6. Yang, I. et al. 2016, 7. Allegretti, J. R. et al 2019, 8. Kim, S.-K. et al. 2019, 9. Schrezenmeir, J. & de Vrese, M. 2001, 10. Senok, A. C. et al. 2005, 11. Walter, J. et al. 2018, 12. Wieërs, G. et al. 2020, 13. Williams, N. T. 2010, 14. Wischmeyer, P. E. et al. 2016, 15. Wilkins, T. & Sequoia, J. 2017, 16. Khoruts, A. 2018, 17. Maldonado-Gómez, M. X. et al. 2016, 18. Zmora, N. et al. 2018, 19. Suez, J. et al. 2018, 20. Choi, H. H. & Cho, Y.-S. 2016, 21. Gupta, S. et al. 2021, 22. Xu, M.-Q. 2015, 23. Aldars-García, L. et al. 2021, 24. Anderson, J. L. et al. 2012, 25. Tan, P. et al. 2020, 26. Allegretti, J. R. et al. 2021, 27. Kootte, R. S. et al. 2017, 28. Proença, I. M. et al. 2020, 29. Rinott, E. et al. 2021, 30. Rinott, E. et al. 2021, 31. Zhang et al. 2019, 32. Huang, H. et al. 2019, 33. Segal, A. et al. 2021, 34. Sun, M.-F. et al. 2018, 35. Kang, D.-W. et al. 2017, 36. Kang, D.-W. et al. 2019, 37. Li, N. et al. 2021, 38. Brandt, L. J. & Aroniadis, O. C. 2013, 39. Zeng, W. et al. 2019, 40. Bojanova, D. P. & Bordenstein, S. R. 2016, 41. Hamilton, M. J. et al. 2013, 42. Khoruts, A. et al. 2010, 43. Severyn, C. J. & Bhatt, A. S. 2018, 44. Weingarden, A. et al. 2015, 45. Aggarwala, V. et al. 2021, 46. Li, S. S. et al. 2016, 47. Smillie, C. S. et al. 2018, 48. Staley, C. et al. 2017.